Table of Content
For incomplete ileus, the success rate of purely supportive treatment is 80%, while the probability that bowel resection will be needed is under 5% . On the other hand, if complete ileus is treated conservatively, the probability that bowel resection will be needed is roughly 30% . Proper treatment depends on the timely determination of the pathogenesis and on close interdisciplinary collaboration. A special challenge is posed by patients with peritoneal involvement with cancer who present with symptoms of ileus, in whom a clear distinction between mechanical and functional causation cannot always be drawn. Ileus is one of the more common suspected diagnoses in everyday clinical practice.
This bag allows stool to drain from your remaining gastrointestinal tract. For example, extensive abdominal surgery is not suitable for some people. An ileus is common after surgery because people are often prescribed medication that can slow intestinal movement. Treatment options for an ileus include waiting for the ileus to resolve, making dietary changes, or adjusting medication use. The treatment depends on the severity of the ileus and its underlying cause.
Spastic colon and constipation
Enter search terms to find related medical topics, multimedia and more. If your rabbit won't take Critical Care or you do not have access to any, grind up rabbit pellets mixed with water, or mixed vegetable baby food as alternatives. Your vet will tell you how much food you should syringe-feed your rabbit, but it will probably be more or less 20–30 ml's twice a day. If your rabbit is eating a little on its own it could be less. Alycia Washington is a Doctor of Veterinary Medicine with nearly a decade of experience as a small animal emergency veterinarian.
Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults. Branco BC, Barmparas G, Schnuriger B, Inaba K, Chan LS, Demetriades D. Systematic review and meta-analysis of the diagnostic and therapeutic role of water-soluble contrast agent in adhesive small bowel obstruction. Cosse C, Regimbeau JM, Fuks D, Mauvais F, Scotte M. Serum procalcitonin for predicting the failure of conservative management and the need for bowel resection in patients with small bowel obstruction. In young, clinically stable patients whose site of blockage is unclear, a so-called MR Sellink study can be performed to localize the problem and facilitate treatment planning.
What is the definition of spastic ileus?
Its main manifestations are bloating (80%), cramps (60%), and retention of stool and flatus (50%). The overt illness is often preceded by a long phase of altered bowel habits and worsening constipation . Outcome measures included time to first passage of flatus, first liquid meal, first bowel movement, and total length of hospital stay.
Patients with POI may experience a painful and distended abdomen, vomiting, toxemia, and dehydration. Although the lumen is not occluded, peristalsis fails when the intestinal contents back up, resulting in watery diarrhea. Pain rarely has the classic colicky pattern present in mechanical obstruction.9 Bowel sounds are minimal or absent. Abdominal tenderness generally is present only when the cause of the ileus is inflammation. The cause of ileus appears to be multifactorial .1,6 POI may result from the use of postsurgical opioid pain relievers (e.g., morphine), which can slow or inhibit normal motility. Opioid analgesics relieve pain by blocking pain signals through stimulation of opioid receptors located on the surface of the nerves that transmit these signals.
Hospital care
Instead, a surgeon may fit a stent into the person’s intestines to keep the intestine open and allow bowel materials to pass through more easily. As a result, you may not have much time to prepare for an appointment. If you have time before your appointment, make a list of your signs and symptoms so that you can better answer your doctor's questions. In cases where the colon is enlarged, a treatment called decompression may provide relief. Decompression can be done with colonoscopy, a procedure in which a thin tube is inserted into your anus and guided into the colon.
Gastrointestinal symptoms are the most common signs of an ileus. Your stomach and intestines will start to fill with gas that can’t pass out the rectum. This causes the abdomen to take on a tight and swollen appearance. The doctor then performs a physical examination to check for swelling or pain in the abdomen. Absent or excessive bowel noises suggest an ileus, although doctors usually require imaging tests to confirm a diagnosis. Methylnaltrexone and alvimopan are promising new agents that could become an important component of perioperative care for the treatment of POI after bowel resection and, potentially, other major abdominal surgeries.
Differential Diagnosis
On the other hand, if the anastomosis fails, the morbidity and mortality rise considerably. 8.Condon RE, Cowles V, Ekbom GA, Schulte WJ, Hess G. Effects of halothane, enflurane, and nitrous oxide on colon motility. Upright position, especially in patients who may have spent a lot of time lying down. Electrical stimulation to encourage movement in the intestine. Your doctor will use a stethoscope to listen to the sounds your belly makes.
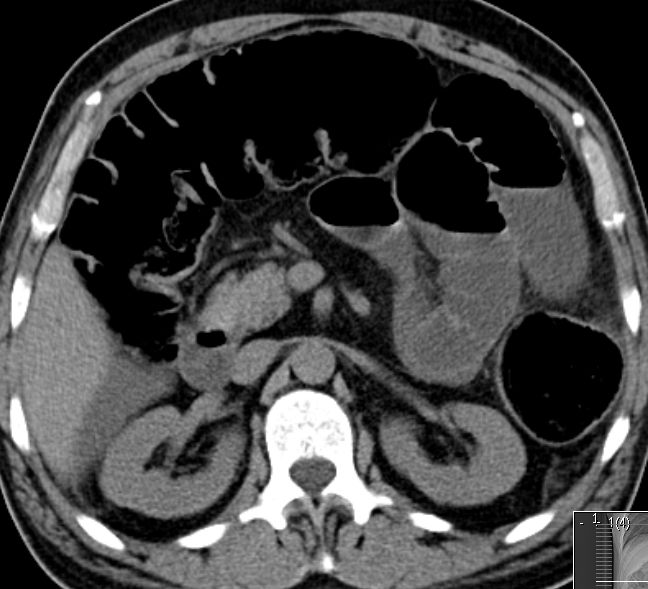
Unlike naloxone, it is a quaternary derivative of naltrexone. The addition of a methyl group at the amine in the naltrexone ring results in a compound with greater polarity and lower lipid solubility; thus, the drug is prevented from crossing the BBB. This allows it to block peripheral receptor opioid effects without altering central analgesic effects. Methylnaltrexone has been shown to antagonize morphine-induced inhibition of contraction in isolated guinea pig ileum and human intestine. Reduction in GI transit time has been observed in subjects with OIC and in healthy opioid-naïve subjects. An x-ray or CT scan may be used to differentiate the type of obstruction versus ileus.
If the obstruction does not clear on its own, you may need surgery to relieve the obstruction. An air or barium enema allows for enhanced imaging of the colon. This may be done for certain suspected causes of obstruction. During the procedure, the doctor will insert air or liquid barium into the colon through the rectum. For intussusception in children, an air or barium enema can actually fix the problem most of the time, and no further treatment is needed. To confirm a diagnosis of intestinal obstruction, your doctor may recommend an abdominal X-ray.
Opioid analgesics bind to the mu receptors in the central nervous system and the GI tract. The binding of opioid analgesics to mu receptors in the GI tract greatly slows intestinal motility, thereby disrupting normal GI function. The slowing of intestinal motility may cause significant discomfort and pain. The combination of both endogenous and exogenous opioids may contribute to the development and persistence of ileus. Increased doses of opioid analgesics are related to extended periods of POI.
The patient must be closely observed both clinically and radiologically, with repeated abdominal plain films every 12 to 24 hours to monitor the diameter of the colon. Magnetic resonance imaging still generally plays no role in the acute evaluation of ileus. Nonetheless, in young, clinically stable patients whose site of blockage is unclear, a so-called MR Sellink study can be performed to localize the problem and facilitate treatment planning . This magnetic resonance version of the Sellink double-contrast study enables the detection of inflammatory/infectious changes or stenoses, particularly of the small bowel. Anyone experiencing symptoms of ileus, including stomach pain, severe constipation, vomiting, and bloating, should seek medical attention.

Prevention of ileus is the responsibility of both the patient and healthcare providers, including, nurses, pharmacologists, and physical/occupational therapists. Encouraging ambulation, enhanced recovery after surgery protocols, and educating the patient on their importance and benefits should improve patient understanding and compliance. Plain abdominal films are usually the first diagnostic imaging obtained. Eliciting the difference between an ileus and a mechanical obstruction, especially if it is only a partial obstruction, can be difficult but is an important distinction to make. Supine and upright films may reveal dilated small bowel loops but should also show air in the colon and rectum without a transition point. If the plain film is vague, a computed tomography scan of the abdomen should be obtained.